Yesterday I completed SimMarathon in Spring in SIMSTAR
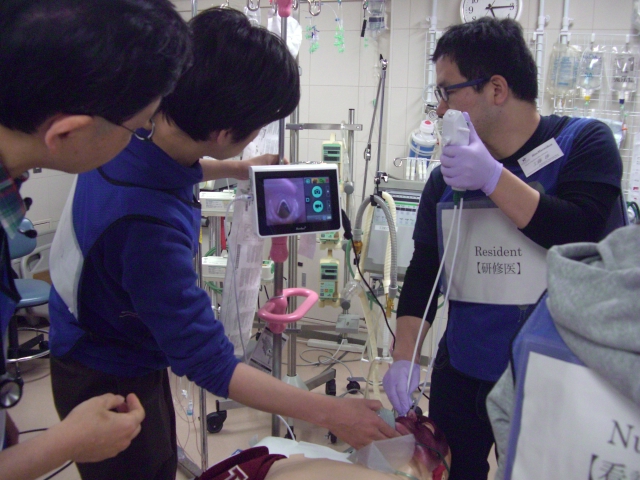
This is 8 hours ER based simulation for both passionate learners and facilitators.
In this simulation seminar, I’m always pursuing reality and authenticity as director.
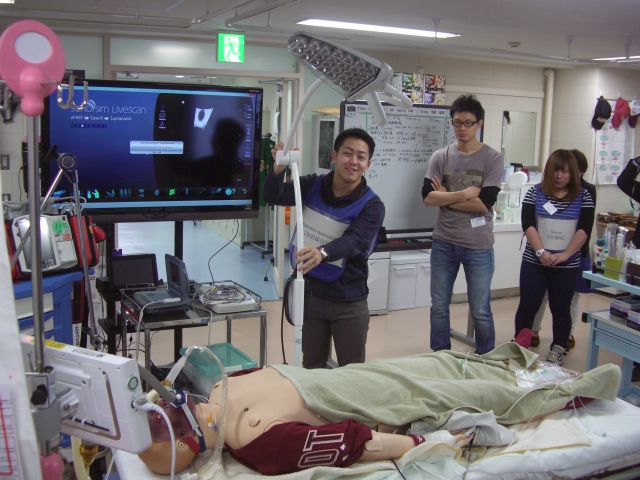
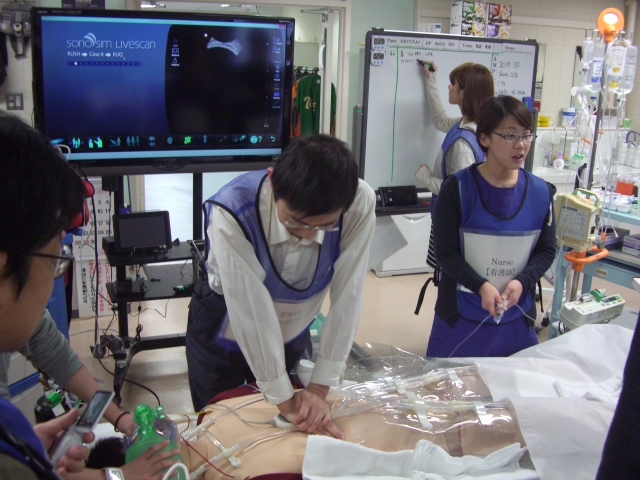
Both real ECMO cannulation and SonoSim Live Scan are special challenges of this simulation. Of course either worked!
SonoSim was efficiently collaborated with prepared scenarios.
Every patient has gotten resuscitated and stabilized by synergy of team dynamics 🙂
Scenarios are as follows;
64 M
CC; burn
Dx; large burn+inhalation injury by house fire, TBSA 66%(head to toe)
PH; n.p.
Tx; Airway control, fluid resuscitation, wound care etc
20 M
CC; syncope, LOC→gasping, VF
Dx; Idiopathic VF, persistent VF
PH; WPW syndrome
Tx; DC many times/adrenaline/amiodarone/intubation → ECPR(PCPS) → rhythm conversion → CT(full body)& CAG, TTM
45 M
CC; faintness, nausea
Dx; profouned bradycardia, hyperkalemia, CKD
PH; HT, DM, DM nephropathy, CKD pre-HD
Tx; Ca, GI, Lasix for hyperkalemia, atropine & TCP for bradycardia
67 M
CC; altered consciousness
Dx; Acute Pancreatitis(alcoholic) with ARDS by CECT, severe shock
PH; alcoholics
Tx; massive fluid resuscitation, ABx, intubation, low tidal volume ventilation for ARDS
16 F
CC; death leap
Dx; unstable pelvic fracture, multiple limb fractures, rt pneumothorax
PH; pregnancy susp
Tx; transfusion of O-type blood and AB-type FFP, pelvic external fixation, PPP→CT→TAE
rt pneumothorax worsening after intubation → needle decompression/chest drainage
53 M
CC; pyrexia, rt leg swelling,pain & erythema, consciousness down
PH; untreated DM
Dx; NSTI with gas of rt. leg, septic shock/DIC
Tx; EGDT, ABx, CECT, not only debriedmant but amputation needed for source control
50 M
CC; syncope, dyspnea, cyanosis
Dx; massive PE/DVT→syncope/shock
Tx; intubation/catecholamine→VA-ECMO(PCPS)→CECT
PH; overweight
64 M
In ICU
CC; desaturation, high airway pressure, cannot ventilate through ETT
Situation; subacute phase of burn, intubated & sedated, mechanically ventilated
Dx; total tube obstruction by sticky and hard sputum
57 M
CC; rigidity of mouth, swallowing disorder(walk-in)
Dx; tetanus,trismus, difficult airway
PH; alcoholics
Tx; cannot ventilate/cannot intubate→TTJV→cricothyroidotomy