手持ちの資料を片付けていたら、2005年にUS Simulation Centerの視察(Laerdal社による企画)に行った時の記録が出てきた。僕がSimulation Educationに没頭するトリガーとなったツアーである。
10年経って、改めてその時に感じたこと、展望(野望?)を振り返ると、「それなりにできていることもあるなぁ」と感じる一方で、その当時のWISERに到達できていないもどかしさも感じる。
その当時の思いは、今シミュレーションで苦労している人に共通する所もあると思うので、ここでシェアしたいと思う。その当時の記録の完全コピーです。ちょっと長いけど、是非読んでみて下さい。




【訪問施設】
1.STRATUS simulation Center(マサチューセッツ州ボストン市)
2.WISER Center(ペンシルバニア州ピッツバーグ市)
【視察期間】2005年3月6日~2005年3月13日(8日間)
【視察の概要】
STRATUS simulation CenterとWISER Centerはともに世界有数のメディカルシミュレーションセンターであり、どちらの施設においても高機能シミュレーターを用いた最先端のシミュレーション教育を展開している。STRATUSは小規模なセンターの代表であり、WISERは世界屈指の大規模シミュレーションセンターである。いずれの施設でも教育対象は医学生、看護学生、レジデント、一般医師、救急救命士と広範囲にわたり、エビデンスに基づいた救急治療をリアルなシミュレーションでトレーニングし、その後の教育効果に関する評価研究も行っている。日本にはこれらのセンターに匹敵するシミュレーションセンターがないため、両センターで展開されているシミュレーション教育コンテンツ、シミュレーションセンター設立のノウハウ、シナリオ作成技術、指導者(インストラクター、ファシリテーター)養成の手法に関して視察を行った。
【STRATUS simulation Center】
STRATUSでは、Dr. ポズナーの指導の下、院内救急・医療の質向上のためのシミュレーション教育と教育効果検証につき研究を行った。特にDr. ポズナーが力を入れて展開しているCrisis Management(緊急危機管理対策)について多くの知見を得た。以下項目別に列挙する。
Dr. ポズナーの所属するBrigham and Women’s Hospitalでは、シミュレーターを使って病院内で抜き打ちの蘇生コードを走らせる。集まったスタッフには倒れたはずの傷病者がシミュレーターであることが判明しても、そのままコードを走らせ、蘇生にいたるように努力させる。シミュレーターにはあらかじめ決まったシナリオがインストールされており、時間以内にやるべき処置を行わないと死亡する。このようなトレーニングを毎月のように行うことで、病院としての緊急時への対策としている。コードに参加したものは、「次はいつやるのか?」というようなことを聞くが、あくまでも極秘スケジュールである。これらはただの「脅し」のトレーニングではなく、蘇生開始までの時間、除細動までの時間、気管挿管までの時間、エピネフリン静注までの時間を計測し、蘇生行為そのものが妥当であったのかどうかを検証している。このようなシミュレーターを用いた蘇生コードトレーニングは、病院の安全管理グループがただ一方的にやり続けても効果的ではない。表裏一体となる教育システムが整備されてはじめてその効果を検証できる。STRATUSはその教育を一手に引き受ける教育施設となっている。
心停止、アナフィラキシーショック、緊張性気胸といった死に直結するイベントは、頻度は圧倒的に少ないものの、ある一定の頻度で発生し得る。これらの稀な病態を実際の臨床現場の症例のみですべての医療スタッフが同じように経験し、かつ常に最善の蘇生行為を行うことは困難である。しかし、このようなことは医療安全の観点から言えば許されるべきことではない。こういった問題を解決するのがシミュレーション教育である。シミュレーターを用いることで、大人数に対して同じ内容の教育を提供することが可能となる。
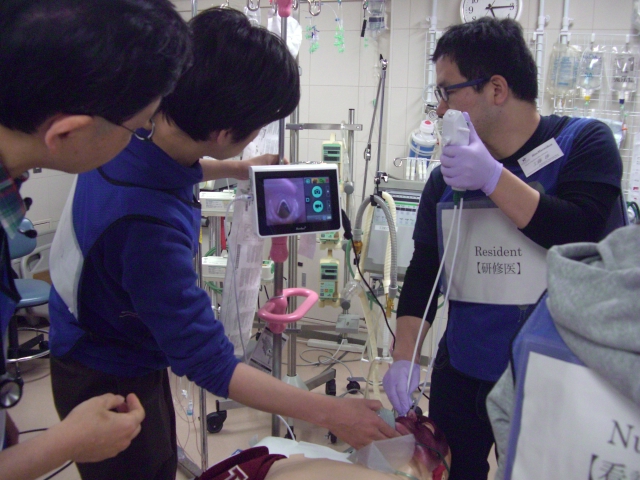
近年の高機能シミュレーターは「ヒューマン・ペイシェント・シミュレーター」と呼ばれ、リアルなシミュレーションが可能となっている。患者評価のパラメーターとしては、いわゆるバイタルサイン(血圧、呼吸、心拍数、動脈血酸素飽和度)などを実際の所見として取ることができ、また気道の状態(喉頭痙攣、開口障害、咽頭浮腫、舌浮腫)、呼吸音(乾性ラ音、湿性ラ音、気道狭窄音など)、心音(収縮期雑音、拡張期雑音など)を変えることができる。行える処置は気管挿管、輪状甲状間膜切開、除細動、経皮ペーシング、気胸の脱気、胸腔ドレーン挿入、静脈ルート確保などがある。一部の心血管作動薬に関しては、あらかじめそれぞれの薬剤投与後のバイタルサインの変動が組み入れられており、薬剤投与のシミュレーションを行うことも可能である。このようなシミュレーターを用いることで、ほぼ臨床の現場に即した模擬患者を創り出すことができる。
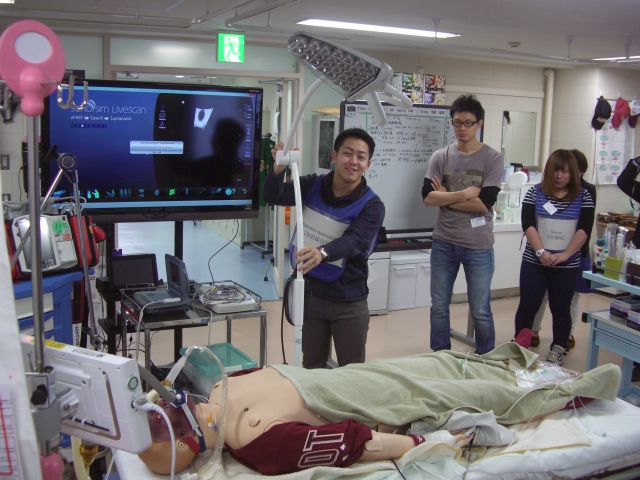
人形だけがリアルでもトレーニングのための環境が整備されていなければ教育効果は上がらない。トレーニングルームを本当の病室や救急外来のように整備し、利用する器具や薬剤などもすべて本物であることが理想的である。本物を用いてこそ臨床に即したシミュレーションが可能となる。こういったトレーニングを「フルスケールシミュレーション」と呼ぶ。シミュレーターの動作ソフトには代表的なシナリオがインストールされていて、適切な時間内に適切な処置を行わないと刻々とバイタルサインが変化し、救命できないようなフローになっている。シナリオは独自に作成することも可能である。
シミュレーションでは、視覚・聴覚・触覚を研ぎ澄ませ、患者の状態を迅速に判断し、適切な処置を行うことが必要であり、講義では決して習得することのできない判断力やスキルを習得することが可能である。仮に判断ミスがあったり処置までの時間が遅れたりしても、シミュレーションゆえ間違いが許され、やり直しが可能である。シナリオ終了後十分なデブリーフィング(反省会)を行えば、ミスをネガティブに捉えるのではなく、次のステップへの糧としてつなげることが可能となる。
このようなシミュレーション教育を継続して行っていくためには、専用の教育施設が必要であり、施設のマネージメントのためには専属の職員が必須である。日本ではシミュレーション教育のための専属スタッフをおいている施設は極めて少なく、種々のタスクトレーナーや高機能シミュレーターを購入し専用の部屋に置いているにもかかわらず、利用頻度が極端に少なく、その存在を知られぬままに埃を被っている施設がある。シミュレーターのメンテナンス、消耗品補充、教育スケジュール調整、事務作業等を専属職員が担当すれば、円滑なシミュレーション教育プログラムの展開を行うことが可能となる。専属職員は臨床経験を有し、指導者としても活躍できる人材であることが望ましい。STRATUSでは現役を引退した救急救命士が専属職員となり、シミュレーションセンターの管理運営を行っている。彼は自らインストラクターとしても活動し、シナリオ作成なども手がけている。
同じシミュレーションでも近年PC上でシミュレーションを行うソフトの開発が進んでおり、このようなPCシミュレーションを「Microsimulation」と呼んでいる。STRATUSではMicrosimulationを利用した教育を十分に活用している。MicrosimulationはPC上とはいえ、実際の症例のダイレクトな反応を評価しながら診断と治療を行うProblem Based Learningであり学習効果は高い。このソフトには様々なシナリオがインストールされており、画面上には実際の救急外来などのシチュエーションが出てきて、チームリーダーとして実際の患者の評価・処置・治療を行っていく。評価・処置・治療は幾つかの項目から選択する。シナリオを終了すると選択した処置が適切であったかどうかのフィードバック画面が表示される。学習者個人で自主学習することも可能であるが、やはりシナリオに精通し、ポイントを外さず指導できるファシリテーターがいると学習効果は更に高まる。ファシリテーター抜きで、ただPC上でシナリオをこなしただけではゲーム感覚で終わってしまう可能性が高く、そこにe-learningの難しさがある。
【WISER center】
WISERでは、Dr. ジョン シェイファーの指導の下、「いかにしてシミュレーションセンターを立ち上げるか」ということに関してのコースに参加し、数多くのノウハウを得ることができた。以下、幾つかのステップで解説する。
まずは教育対象がどのような集団であるのかを把握することから始まる。一般的に救急医療従事者が多くなるが、最近では市民もその対象となりうる。
【教育対象例】
救急隊、救急救命士、看護学生、看護師、医学生、研修医、臨床医、一般市民
- ステップ 2;「それぞれの教育対象に対してどのようなコースを開催するかを決める。」
あらゆる対象に共通したコースもあるが、それぞれの職種のニーズに合わせた専門的なコースも提供していく必要がある。
【対象別教育内容の例】
救急隊 ;BLS/ACLS/外傷診療、基本的気道管理手技、脳血管障害の初療
救急救命士 ;BLS/ACLS/外傷診療、基本的気道管理手技、困難な気道の管理手技、
脳血管障害の初療、危機管理マネージメント
看護学生 ;BLS/ACLS/外傷診療、ベッドサイド手技、ICUオリエンテーション
看護師 ;BLS/ACLS/外傷診療、ベッドサイド手技、基本的気道管理手技
医学生 ;BLS/ACLS/外傷診療、臨床診断技術、不安定患者へのアプローチ
ベッドサイド手技、基本的気道管理手技
研修医 ;BLS/ACLS/外傷診療、ベッドサイド手技、困難な気道の管理手技
気管支鏡トレーニング、危機管理マネージメント、コードチーム
トレーニング、麻酔のイントロダクション
臨床医 ;BLS/ACLS/外傷診療、コードチームトレーニング、小児の危機管理
マネージメント、困難な気道の管理手技、集団災害
一般市民 ;BLS、ミニ医学講座
- ステップ 3;「リアルなトレーニングを行うためにふさわしい環境・設備を整える。」
“他人のゴミは、自分にとっては宝物かも知れない。” 中古品や期限切れ品などを再利用するルートを作り、無駄な投資をしないように工夫をすることが重要である。不要となったベッド、ストレッチャー、点滴台、点滴ポンプ、テーブル、机、椅子などはできるだけ利用する。全てが新品である必要はない。コンピューターなどはターンオーバーが早いため、少々古い機種でもウェブの閲覧用としては十分に再利用可能なものが多い。医療資材は期限切れや、一度開けたけど使用しなかったものなどを回収すれば立派にトレーニング用に用いることができる。薬剤なども使用済みのシリンジに水を入れておけば、シミュレーションでは十分にその役割を果たす。その他の戦略としては、病院の医療安全グループと組むことが推奨される。トレーニングの重要性を理解してもらえれば新規の器材購入の予算確保が可能となるかもしれない。また企業と提携していくのも一つの方法である。宣伝を目的としてサンプルを無料で提供してもらうことが期待できる。この場合、限定した企業に偏ることなく、あらゆる企業の協力を受ける必要がある。
【必要設備例】
手術室 ;手術台、麻酔器、モニター類、薬剤カート、外科手術用具、吸引
ICU ;ICUベッド、人工呼吸器、モニター、点滴ポンプ、救急カート、吸引
一般病室 ;入院ベッド、限られたスペース
講義室 ;十分な広さ、椅子、テーブル、AV機器、ホワイトボード
- ステップ 4;「受講生のニーズに見合ったコースを実際に開催できるのかどうか、論理的に考慮する。」
あるグループに対して、あるモジュールのコースを開催するとき、どれだけの人数をどれだけの期間で教育することができるのか、ということを計算してプログラムを組む必要がある。まずは限られたスペースで実際に開催できるだけのコースを企画していかないと、コースの質が低下し、センターの評判を落とすことになる。
- ステップ 5;「教育手法的に効果の上がるスペース作り、フィードバック方法を考える。」以下のような環境整備を検討する。
【スライドプロジェクター】
部屋の広さによらず、全てのトレーニングルームにプロジェクターと投影用のスクリーンを用意することが望ましい。こうすることでどの部屋でもパワーポイントを用いたレクチャーや、プロジェクターを通したウェブの閲覧、ビデオによるデブリーフィングが可能となる。
【インターネット環境】
全てのシミュレーションルームにインターネットを配信できるように、ウェブ環境を整えることが理想的である。WISERでは各コースの教材をWISERのホームページにアップロードしているため、そこにアクセスすることでどの部屋でも容易に教材を閲覧できる。
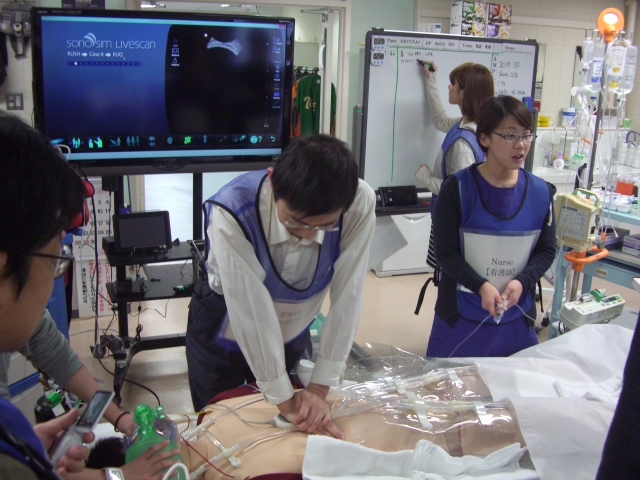
【ビデオカメラレコーディング】
全ての部屋にビデオカメラを設置し、シミュレーションを録画できれば、より効果的なフィードバックが可能となる。WISERでは、シナリオの開始とともにVTR録画がスタートし、シナリオ終了直後に、行った処置の経過記録一覧をプロジェクターで提示し、修正点(赤字で表記)については経過記録一覧のその部分をワンクリックするだけで同時刻のVTRの頭出しが行われ、ビデオによるフィードバック(部屋によっては2方向で録画)が可能となっている。
【ケーブルレス】
PCも無線LANやケーブルレスのマウス・キーボードを使うなどして、ケ-ブルによる煩雑さを避けると器材の管理が容易となる。
- ステップ 6;「限られた環境でも、そこで最大限可能な教育を始め、指導者を育成する。」
シミュレーターやその他の環境は教育のための一つの道具であり、ただシミュレーターを置いた部屋を確保しただけではまったく意味を成さない。重要なのは展開される教育コンテンツ(シナリオ)のクオリティと、受講生のパフォーマンスを適切かつ迅速にフィードバックできるインストラクターやファシリテーターの能力や情熱となる。こういった教育に情熱のある人材を発掘・育成し、参画してもらうことこそが最大の課題である。小規模でもよいので、できることから始めなくてはその先の発展はない。
【総 括】
院内救急システム構築のみならず、広く「Save Lives」という大きなミッションを達成するためには、シミュレーション教育は今後必須のツールであることは間違いない。WISERセンターにおけるシミュレーション教育のシステムは非常に完成度が高く、シナリオ作成、インフラ整備、スタッフ教育、ビジネスモデルに至るまで全てのノウハウを日本でも十分に活かす必要がある。注意すべきは、WISERセンターのような大きなシミュレーションセンターがあちこちに乱立するのは賢明なことではなく、大学病院を中心として核となるシミュレーションセンターを地域にいくつか作り、それらの運営ノウハウを分かちあう形で、地域病院単位ではSTRATUSのような小規模なセンターを整備していくのが理想的である。