“SimNight” is one of my original simulation seminars.
As you notice, the name comes from “Simulation at Night”.
I have been doing this scenario-based simulation since 2012 in my simulation center.
Literally this seminar would be held from 7pm to 9pm mostly on Tuesday.
Participants who are healthcare providers like doctors and nurses come voluntarily from both my hospital and other institutions.
Surprisingly this seminar is free in charge, therefore it is very easy to apply and join.
Every time I provide 2 or 3 comprehensive scenarios related to the emergency medicine such as cardiovascular failure, respiratory failure, sepsis, trauma, poisoning and environmental disorder. Realism is the strongest point of my seminar.
Yesterday, I did “SimNight” seminar for the first time in about 2 months.
Participants who joined today’s seminar flew from Shizuoka that is far from my city.
I was surprised at the level of performance which they did as a team in these scenarios.
___
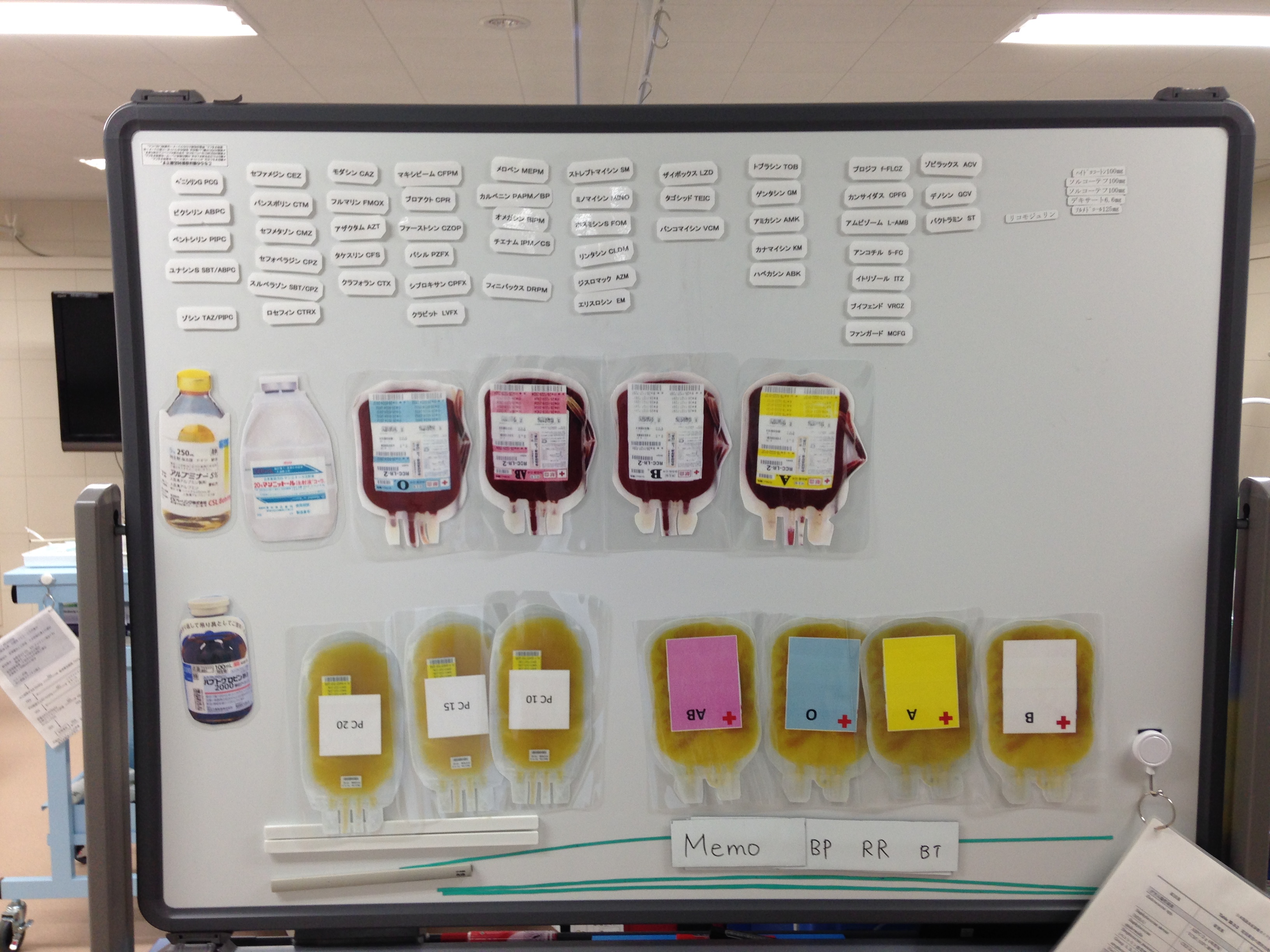
SimNight scenarios on 2015/2/3
53M
CC: pyrexia, rt leg swelling,pain & erythema
PH: DM not treated
by ambulance
Condition: NSTI of rt. leg with abnormal gas, septic shock/DIC→EGDT, ABx, CECT, debriedman to amputation
53M
CC: organophosphate poisoning
PH: HT, HL, depression
by ambulance
Condition: miosis, fasciculation, airway emergency by secretion → intubation, atropine + PAM
19M
CC: blunt trauma, rt. chest pain
PH: n.p.
by ambulance
Condition: rt tension pneumothorax, lung contusion, aortic injury, hepatic injury → needle decompression, chest tube, CECT, intubation, Angio
57M walk-in
CC: rigidity of muscles around mouth and neck, swallowing disorder
PH: alcoholics
Condition: tetanus,trismus, difficult airway→emergent cricothyrotomy